Acute coronary syndrome
Acute coronary syndrome
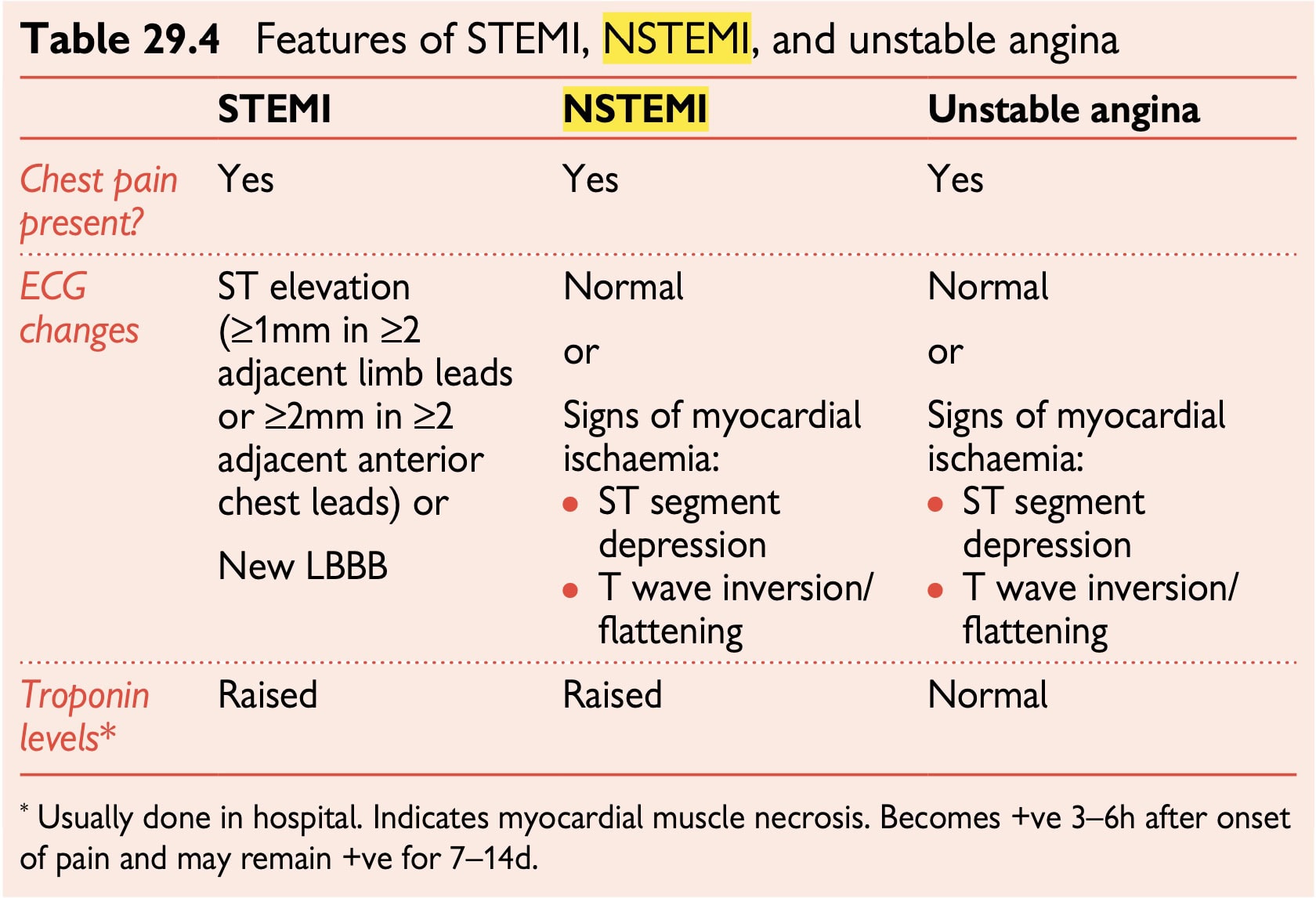
The term acute coronary syndrome (ACS) covers
1- Myocardial infarction Both ST-segment elevation MI (STEMI)
2- Non-ST segment elevation MI (NSTEMI)
3- Unstable angina
Initial primary care management is the same for STEMI, NSTEMI, and unstable angina.
Presentation Maybe new onset or a rapid deterioration in stable angina.
Presenting features
Sustained central chest pain —typically described as central crushing/pressure, band-like pain
Pain radiating to the arms, jaw, back, or upper abdomen (maybe the only symptom)
Symptoms resulting from sympathetic autonomic stimulation, e.g.
nausea, vomiting, sweating
Symptoms relating to shock, e.g. breathlessness, hypotension, collapse
Emergency management
When the call for assistance is made If ACS is suspected, arrange immediate transfer to the hospital. For reperfusion interventions (thrombolysis or percutaneous coronary intervention) to be effective, they must be carried out as soon as possible after the onset of pain. Seeing the patient before arranging transfer introduces unnecessary delays.
If possible attend to the patient once the ambulance has been called: •
Give pain relief with either sublingual GTN or IV/IM opioid (e.g. morphine 5–10mg—half dose if elderly/frail) or both
- Give aspirin 300mg PO (unless contraindicated)
- Consider giving IV/IM antiemetic (e.g. metoclopramide 10mg)
- Measure oxygen saturation with pulse oximeter—only give oxygen if saturations are <94%. Aim for saturations of 94–98% (88–92% if known COPD and at risk of CO2 retention)
- If bradycardia, consider giving atropine 500 micrograms IV and further doses of 500 micrograms if needed to a maximum of 3mg.