Ischemic heart disease
ISCHAEMIC HEART DISEASE
Myocardial ischemia develops when there is an imbalance between the supply of oxygen and the myocardial demand.
ETIOLOGY
1 -Decreased coronary blood flow due to a mechanical obstruction such as:
Atheroma – occluding one or more major coronary arteries.
Spasm of coronary artery
Thrombosis
Embolus
Coronary arteritis (e.g. in SLE)
Congenital abnormalities of the coronary artery.
2 – Increased myocardial oxygen requirement
Increased cardiac output: in thyrotoxicosis
Myocardial hypertrophy: usually from aortic stenosis or hypertension.
3 –Decreased flow’ of oxygenated blood to the myocardium
Anaemia
Hypotension — causing decreased coronary perfusion pressure.
Cardiac syndrome X
The most common cause of myocardial ischemia and angina is the formation of atheroma. Atheroma is a fibrofatty plaque in the intima of large and medium-sized arteries producing narrowing of the lumen of the vessels. The exact cause of atheroma formation is not known.
RISK FACTORS FOR ATHEROSCLEROSIS
Risk factors for atherosclerosis may be fixed or modifiable
Fixed risk factors
Age; – Risk increases with age, rare at a young age except in familial hyperlipidemia.
Male sex. –Men have a higher incidence of ischemic heart disease than premenopausal women. After menopause, the incidence of atherosclerosis in women reaches that in men. This protection in premenopausal women is probably due to estrogen.
Family history: — A positive family history means ischemic heart disease in first-degree relatives before the age of 45 years in males and before 50 years in females.
Modifiable risk factors
Hyperlipidemia;
High serum cholesterol especially increased low-density lipoprotein (LDL) and decreased high-density lipoproteins (HDL) is strongly associated
with coronary atheroma.
Hypertension
Cigarette smoking
Diabetes mellitus
Obesity: particularly central or truncal obesity.
Lack of exercise: regular exercise for 20 minutes 2-3 times/week protects from coronary heart disease.
Heavy alcoholism:
Dietary factors: diet deficient in fresh fruit, vegetable, and polyunsaturated fatty acids are associated with an increased risk of coronary artery disease.
Low levels of vitamin C, vitamin E, and other antioxidants may enhance the production of oxidized LDL that is an important risk for coronary artery disease.
Oral contraceptives
Gout.
Infection with chlamydia pneumonia,
Helicobacter pylori and CMV.
High level of coagulation factor VII and fibrinogen.
Elevated plasma homocysteine level. Folic acid in low doses may prevent its atherogenic effect.
Raised C-reactive protein (CRP).
High plasma lipoprotein (a).
NON-ATHEROSCLEROTIC CAUSES OF CARDIAC ISCHEMIA
1 . Embolism: the source of emboli maybe
Infective endocarditis
Mural thrombi in left atrium or ventricle
Thrombi from prosthetic valves
Intracardiac tumours
Paradoxical emboli from the venous system across ASD or VSD.
2 . Chest wall injury: causing injury to coronary arteries resulting in intracoronary thrombosis.
3 . Mediastinal radiations: causing fibrosis of coronary arteries.
4 . Aortic dissection: may propagate to the aortic root and occlude coronary artery at its origin.
5 . Coronary artery dissection in angiography or angioplasty.
6 . Vasculitis: syphilis, Takayasu’s arteritis, polyarteritis nodosa, SLE, giant cell arteritis, Kawasaki’s ‘disease resulting in a coronary aneurysm.
7. Blood disorders causing intracoronary thrombosis:
Polycythemia vera, DIC, sickle cell anaemia.
8 . Congenital coronary anomalies
9 . Spontaneous coronary spasm: with or without underlying coronary artery disease.
10 . Mismatch of myocardial oxygen supply and demand
- Thyrotoxicosis
- Aortic stenosis
- Aortic regurgitation
- Tachyarrhythmias
- Sepsis
11 . Decreased oxygen delivery
- Acute blood loss
- Hypotension
- Anaemia
- Carbon monoxide poisoning
CORONARY ARTERY DISEASE
Coronary artery disease is the most common cause of death. It is almost always caused by atheroma and its complication such as thrombosis. There are certain presentations of coronary artery disease such as:
1 . Stable angina
- Unstable angina
- Myocardial infarction
- Heart failure
- Arrhythmia
- Sudden death
ANGINA PECTORIS
Angina pectoris is a clinical syndrome characterized by paroxysmal chest pain due to transient myocardial ischemia. It may occur whenever there is an imbalance between myocardial oxygen supply and demand. The most common cause is atherosclerosis; however, angina may also develop in aortic stenosis (AS) and hypertrophic cardiomyopathy (HOCM) even there is no coronary atheroma.
PATHOPHYSIOLOGY
Stable angina:
Stable angina is angina that occurs when coronary perfusion is impaired by fixed or stable atheroma of coronary arteries i-e patient has fixed
the capacity of exertion after that he starts feeling chest pain.
Unstable angina:
Unstable angina is angina that is characterized by rapidly worsening chest pain, pain on minimal exertion, or pain at rest. The culprit lesion is usually a complex ulcerated or fissured atheroma with adherent platelet-rich thrombus and local coronary spasm.
Myocardial infarction
Pathophysiology of unstable angina and myocardial infarction is the same (i-e thrombus formation on atherosclerotic plaque) however in unstable angina obstruction of the artery is incomplete while in MI there generally is total obstruction.
TYPES OF ANGINA
1-Classical or exertional angina
It occurs due to increased myocardial oxygen demand during exertion or emotion in a patient of narrow coronary arteries. It is relieved promptly by
rest and by nitroglycerine.
- Variant or Prinzmetal’s angina
It occurs at rest and is not a result of increased myocardial demand. It is produced by the episodic reduction of myocardial blood supply due to
coronary artery spasm. The underlying atherosclerotic disease may or may not be present. This type of angina occurs more frequently in women (under age 50 years) especially early in the morning, awakening patients from sleep and the pain is usually more severe and more prolonged than in
classical angina. It tends to involve the right coronary artery. It is characteristically associated with ST-elevation rather than depression (as seen in
classical angina).
- Unstable angina
Unstable angina refers to the angina of recent onset (less than one month), worsening angina characterized by increased frequency and duration
of the episode, or angina at rest not responding readily to therapy.
4- Decubitus angina
This is angina that occurs when the patient lies down. It usually occurs in association with impaired left ventricular function. Patient with this
symptoms usually have severe coronary artery disease.
- Nocturnal angina.
This is angina that awakes the patient from sleep. It may be provoked by vivid dreams. It may occur due to critical coronary artery obstruction or
coronary spasm.
- Cardiac syndrome X
The patient presents with angina, a positive exercise test (ETT), and angiographically normal coronary arteries. It may be because of functional
abnormalities of coronary microcirculation (no dilatation of arterioles at the time of stress).
CLINICAL FEATURES OF STABLE ANGINA
SYMPTOMS
Chest pain
Dyspnea
Associated symptoms
Typical angina pain
Pain may arise in one of the following sites.
- Middle or lower sternum (mostly)
- Left precordium
- Epigastrium
- Left shoulder or left upper arm
- Lower jaw
- Interscapular region
Pricking pain for few seconds especially near the left nipple is very common and usually non-cardiac.
Pain can radiate to any dermatome from C8 to T4, it radiates most often to the left shoulder and left arm, moving down to the elbow and ulnar aspect of
the forearm. It may also radiate to
- Left shoulder, both arms
- Back of neck
- Lower jaw
- Interscapular region
- Eigastrium
The patient feels tightness in the chest “like a band around the chest” while describing he commonly laces the hand or clenched fist n the sternum (fist sign). He may also describe it as a sense of pressure, choking, or heaviness in the chest. The pain may be sharp and piercing.
Anginal pain lasts only a few minutes, less than 30 minutes but mostly it remains for 1-4 minutes. It subsides completely without residual discomfort.
Aggravating (precipitating factors)
Physical exertion e.g. exercises, sexual activity.
Heavy meals
Intense emotions e.g. stress, anger, fright, or frustration.
Lying flat (decubitus angina).
Violent dreams (nocturnal angina).
Pain may occur at rest such as variant and unstable angina.
Dyspnea
Associated symptoms
The feeling of uselessness in the limbs
Dizziness or fainting
Choking sensation in the throat
Polyuria after an attack.
SIGNS
During the attack, the patient looks anxious. Dyspnea, pale face, and cold sweats may also be present. In between attacks, the physical examination is frequently negative except for findings of risk factors.
Search for the evidence of the following:
Risk factors: e.g. hypertension, hyperlipidemia (such as tendon xanthomas), diabetes, myxoedema.
Contributory factors: e.g. obesity, anaemia, thyrotoxicosis, and aortic valve disease.
Left ventricular dysfunction such as gallop rhythm, cardiomegaly, and basal crepitations.
Generalized arterial disease e.g. carotid bruits, peripheral vascular disease.
Investigations
- EGG
During pain, ECG shows ST-segment depression with or without T wave inversion that reverses after ischemia disappears.
Elevation of ST-segment in prinzmetal’s angina.
The resting ECG may be normal between attacks however it may show old myocardial infarction, heart block, or left ventricular
hypertrophy.
Stress test
CT angiogram
Coronary angiography
Management
Modification of risk factors after MI
Secondary prevention:
Cholesterol Medications
All patients with proven CHD benefit from a decrease in total cholesterol and LDL, irrespective of initial cholesterol concentration. A decrease in total cholesterol and LDL by 25–35% using statin therapy results in 25–35% decrease in CHD mortality.
β-blockers
Unless contraindicated, start all patients on an oral β-blocker (e.g.atenolol) soon after MI and continue indefinitely. Estimated to prevent 12 deaths/1,000 treated/y. If β-blockers are contraindicated, a rate-limiting calcium channel blocker (e.g. diltiazem or verapamil) is an alternative
ACE inhibitors
Long-term ACE inhibitors: trials show a decrease in mortality for all patients. If ACE inhibitors are not tolerated, use ARB instead.
Antiplatelet medication
Aspirin Starting aspirin 75mg od
Clopidogrel 75mg od—prescribe in addition to aspirin for 12 months following STEMI with drug-eluting stenting
Anticoagulation is Occasionally required if AF, left ventricular aneurysm or if clopidogrel/aspirin are not tolerated.
Routine exercise testing (usually before discharge from hospital) identifies those likely to have angina post-MI who might benefit from early angiography ± angioplasty/stenting or CABG.
Cardiac rehabilitation d risk of death by 20–25%. Provided by specialist multidisciplinary teams. Components include psychological support, information about CHD, structured exercise program, and modification of other risk factors.
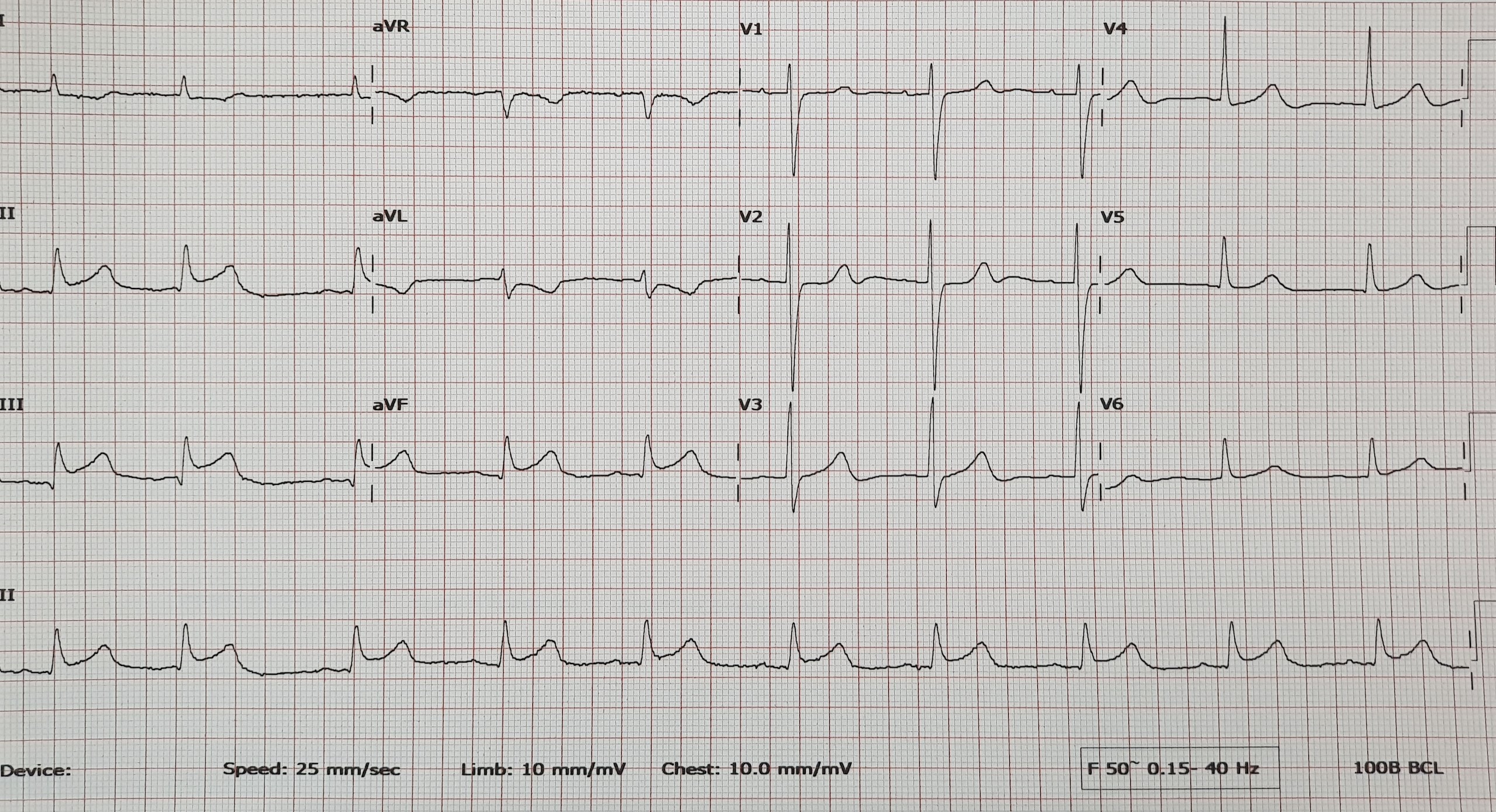
Inferior STEMI