
Hypopituitarism
HYPOPITUITARISM
ETIOLOGY
The causes of hypopituitrarism are best classified on the basis of whether the lesion is in the hypothalamus or in the pituitary gland.
Hypothalamus
1. Congenital isolated deficiency of pituitary
hormones (Kallmann’s syndrome)
2. Acquired
• Craniopharyngioma
• Tuberculosis
• Head injury, surgery
• Radiotherapy
• Tuberculosis, sarcoidosis, histiocytosis
• Syphilis
• Encephalitis
• Primary or secondary tumour
Pituitary
1. Pituitary tumours. Chromophobe adenoma (commonest cause)
2. Surgery, radiotherapy, head injury
3. Post-partum necrosis (Sheehan’s syndrome)
3. Autoimmune.
4. Hemorrhage in pituitary tumour (apoplexy).
CLINICAL FEATURES
Congenital defects of the hypothalamus: thee is an isolated failure of production of releasing hormone e.g. gonadotrophin-releasing hormone causes failure of LH & FSH production and hence failure of sex hormone production. The condition is mostly associated with anosmia. Congenital defects usually present with short stature.
Pituitary lesion (esp. pituitary tumour): there is the sequence of loss of pituitary hormones as following:
Growth hormone loss
Growth hormone is usually the earliest to be lost, it
presents as lethargy, muscle weakness, and
increased fat mass but these features are not much
obvious in adults.
FSH and LH loss
It s the second hormone to be lost, it results in failure of sex hormones production) manifesting as:
• Loss of libido, and importance in male and oligomenorrhoea or amenorrhoea in female.
• Later gynecomastia and decreased frequency of shaving. Axillary and pubic hair become decreased or even absent in both sexes.
• Wrinkled dry skin.
ACTH loss
• ACTH loss results in cortisol deficiency, producing symptoms of secondary adrenal insufficiency (hypotension, hypoglycemia & nausea & vomiting).
• Skin pallor due to lack of melanin in the skin (in contrast to primary adrenal insufficiency in which hyperpigmentation occurs).
TSH loss
TSH loss causes secondary hypothyroidism (hypothermia, low metabolic rate, dry skin,
constipation). Frank myxedema is not seen in secondary hypothyroidism.
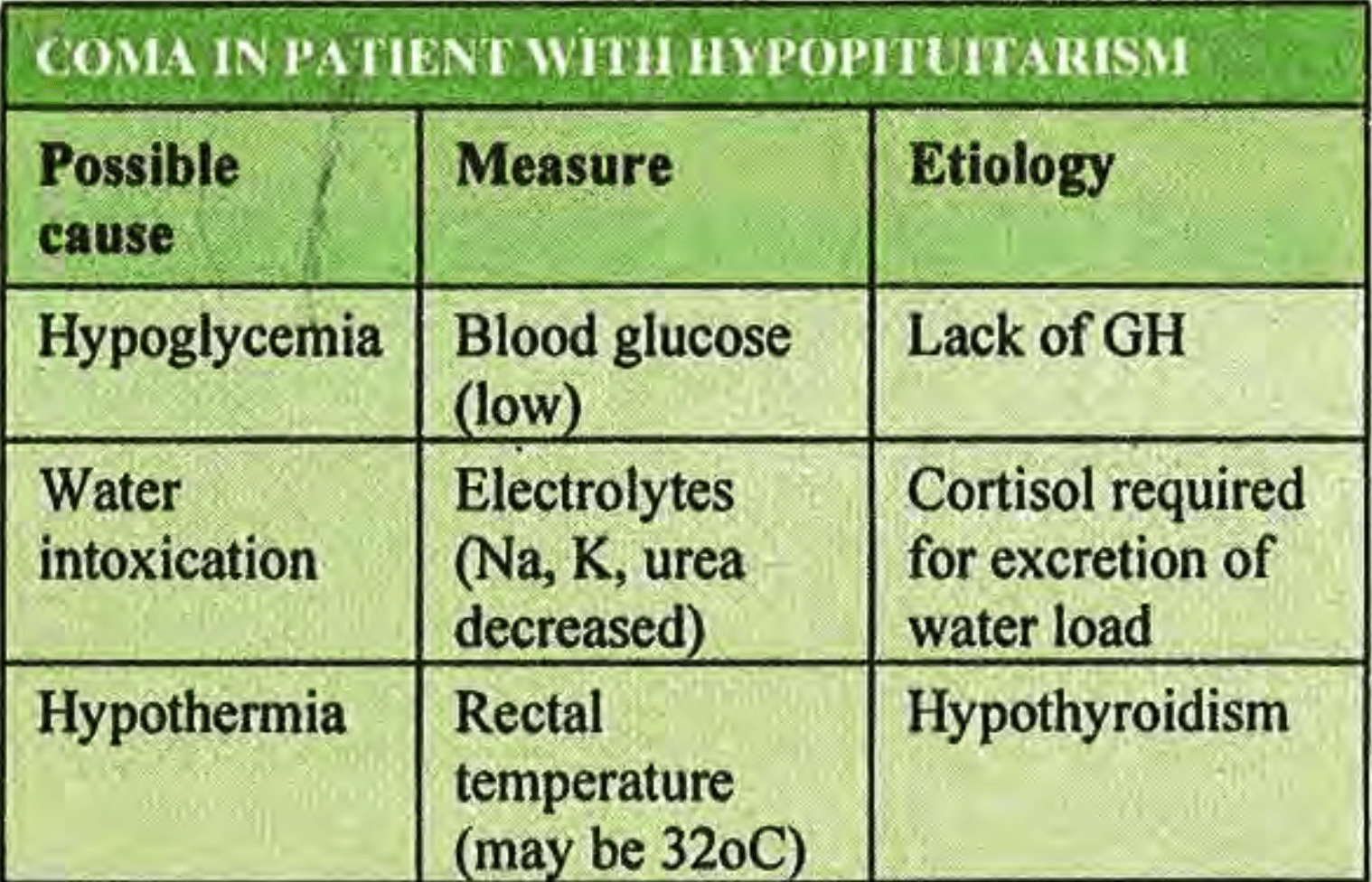
Coma
Patient with untreated severe hypopituitarism eventually goes into a coma, especially after some infection or injury.
Investigations
1. X-ray skull: may demonstrate enlargement of sell turcica due to tumour and suprasellar calcification in craniopharyngioma.
2. . MRI scan of the brain
Pituitary function tests:
Testosterone
Cortisol or (ACTH) adrenocorticotrophic hormone.
Prolactin
Plasma (FSH) follicle-stimulating hormone, and (LH) luteinising hormone.
T,3 T,4
Growth hormone