Pneumonia
Pneumonia
TYPES
1 . Community-Acquired(primary) pneumonia (typical or atypical pneumonia)
2 . Hospital-Acquired (nosocomial) pneumonia
3 – Aspiration pneumonia
4 – Pneumonia in the immunocompromised host including AIDS.
COMMUNITY-ACQUIRED PNEUMONIA
It occurs in previously healthy individuals.
The presentation may be typical or atypical.
Bacterial
Streptococcus pneumoniae
Mycoplasma pneumoniae
Haemophilus influenza
Chlamydia pneumoniae
Chlamydia psittaci
Legionella
Staphylococcus aureus
Coxiella
Viral
Influenza
Parainfluenza,
Respiratory syncytial virus
Depending upon the causative organisms, rapidly of onset, clinical and radiographic evaluation, and laboratory findings, this community-acquired pneumonia can be divided into typical and atypical pneumonia. This designation of “Typical” & “Atypical” is very helpful in providing clues to the possible causes.
Typical pneumonia causes
Streptococcus pneumonia (a most common cause of pneumonia)
Atypical pneumonia causes
Mycoplasma pneumoniae
Legionella
Chlamydia pneumoniae
Viral pneumonia
Coxilla
Typical Pneumonia clinical features
Fever
Chills
Productive cough with purulent sputum
Chest pain
Signs of consolidation such as
Decreased chest movements
Dullness on percussion
Increased vocal fremitus,
Bronchial breath sounds
Crepitations.
Atypical Pneumonia clinical features
Non- pulmonary features are predominant such as
Gradual onset of fever
Dry cough
Myalgia
Arthralgia
Headache
Sore throat
Nausea, vomiting
Diarrhoea
Respiratory symptoms (chest pain, productive cough) are less marked as
compared to typical pneumonia.
Investigations
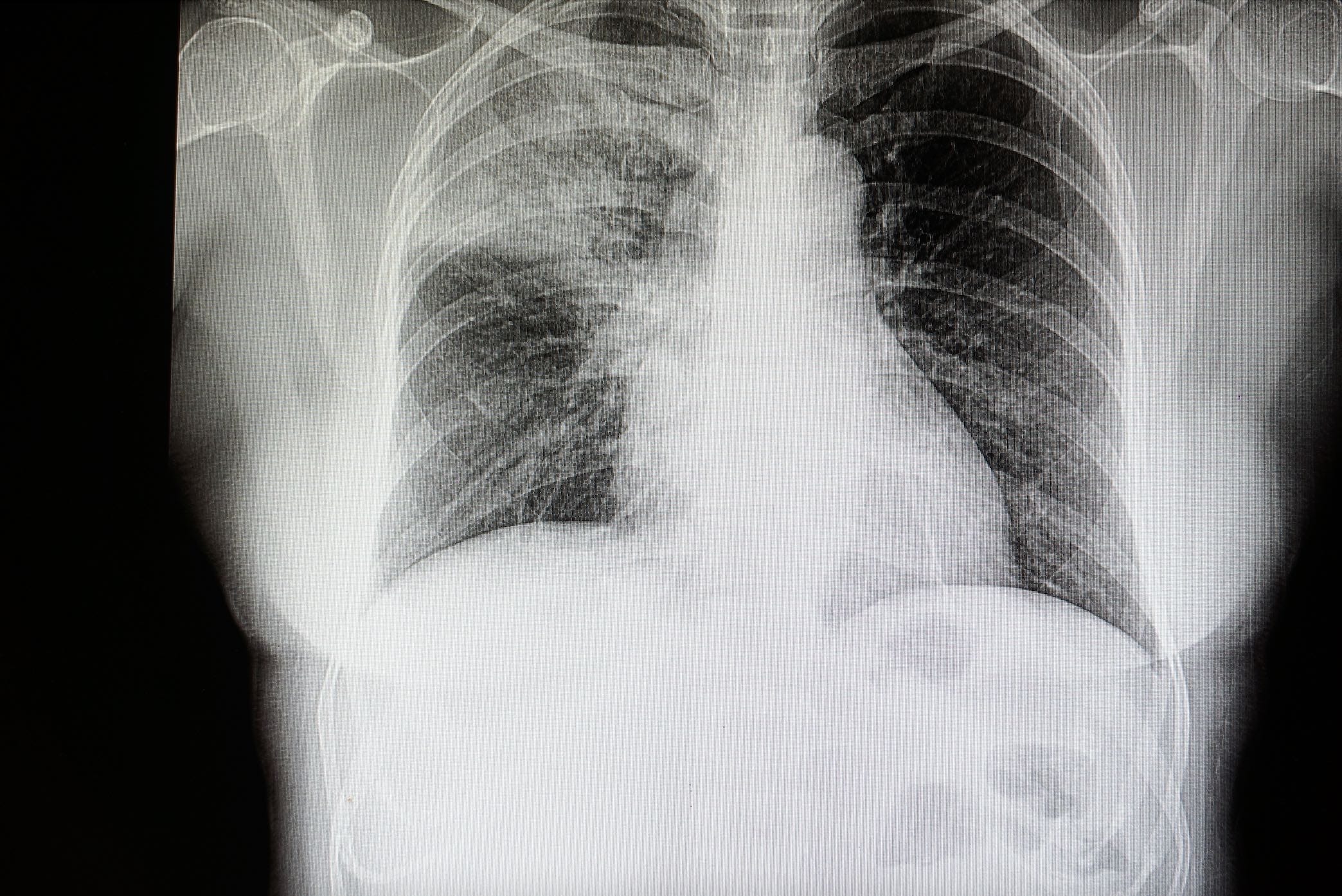
Chest x-ray Typical pneumonia — Patchy or lobar infiltrate (opacity)
Chest X-ray Atypical pneumonia — Patchy non- lobar infiltrates
This is necessary for confirmation of diagnosis and for early detection of complications e.g. pleural effusion and empyema.
Radiological changes lag behind the clinical course so that x-ray changes may be minimal at the start of the illness. Usually, radiological changes appear 12-18 hours after the onset of illness. Conversely, consolidation may remain on the chest x-ray for several weeks after the patient is clinically cured. However, a chest x-ray should always return to normal by 6 weeks. Persistent changes on chest x-ray after this time suggest a bronchial abnormality, usually a carcinoma, with persisting secondary pneumonia.
X-ray chest may show patchy or homogenous opacity localized to the affected lobe or segment. However, the pattern of radiographic abnormalities is not specific to any particular cause of pneumonia.
FBE/ESR
Blood Culture
Serological tests
Pneumococcal antigen test. Serologic test of sputum, urine, and serum for pneumococcal antigen is 3-4 times more sensitive than sputum or blood cultures.
Serological tests (for atypical pneumonia) may be helpful in the diagnosis of mycoplasma, Legionella, chlamydia, and viral infection. A four-fold rise of antibody titer suggests recent infection.
Arterial blood gas measurement – Measured in the seriously ill patient.
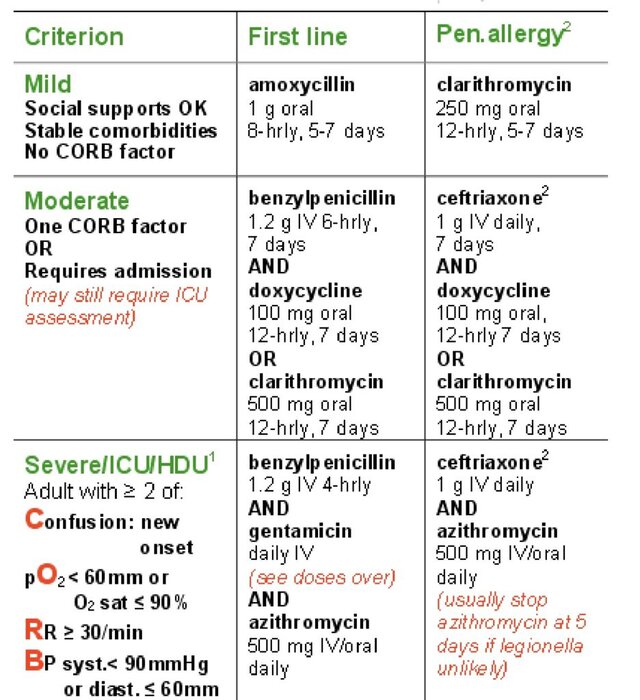
MANAGEMENT
Admit to hospital / Outpatient treatment- Depends upon the severity of pneumonia
Analgesics for pleural pain
Antibiotics